ARF :Causes
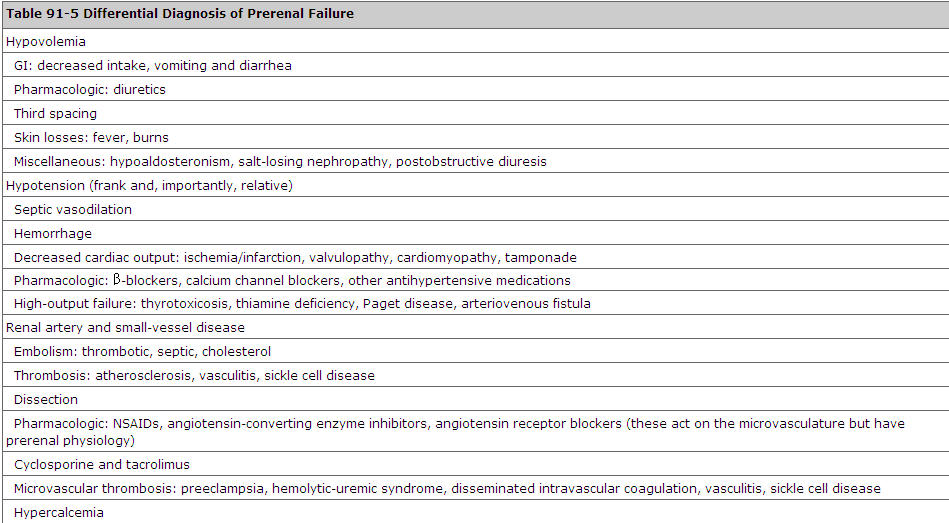



Source:Tintenelli 7th
The informations needed when you want to call 999
ETHANE
E :exact location
T:type of incident
H:Hazards
A-Access block
N:Number of victim
E:Existing of EMS at site


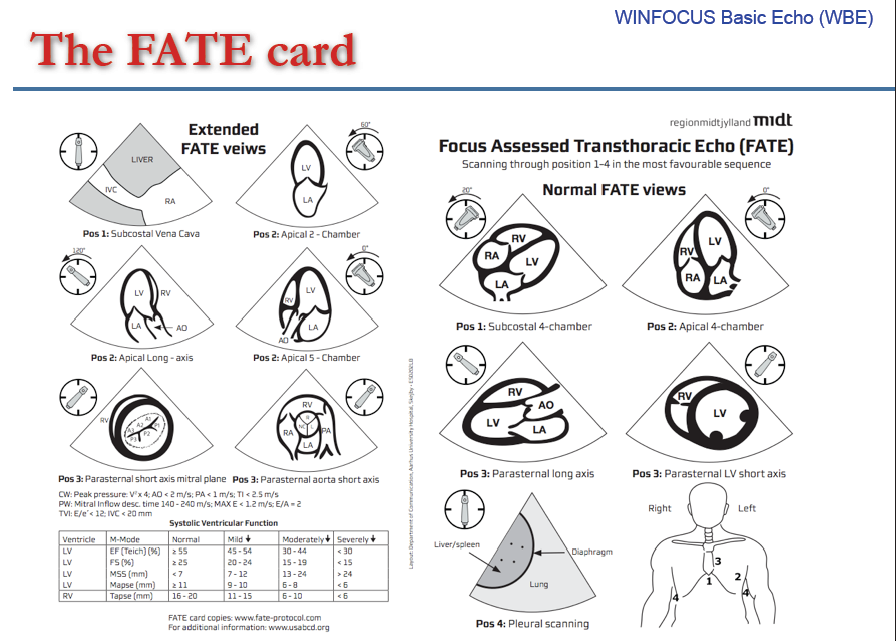
Source:http://sonoguide.com/cardiac.html
1-Anterior septal
2-Anterior free wall
3-Lateral wall
4-Posterior
5.Inferior
6-Inferoseptal
Source:http://lifeinthefastlane.com/education/investigations-tests/urea-creatinine-ratio/ The relationship of urea and creatine is dependent on serum laboratory units used to determine the cause of acute kidney injury. Therefore two ratio’s exist to compare serum Urea and Creatinine levels

The patient is placed in the supine position after
provision of analgesia with or without sedation. The
affected arm is gently lift vertically by grasping
around the wrist. When the affected arm is in
vertical position, vertical traction is applied. While
maintaining the vertical traction, the shoulder is
externally rotated. (Figure 1) A clunk is heard or
felt as reduction occurs.
Tintenelli 7th:
When DKA is suspected, initial steps should include a test-strip glucose determination, a urine test strip, an ECG, venous blood gas determination, and a normal saline (NS) IV infusion.
A blood glucose level >250 milligrams/dL, an anion gap >10, a bicarbonate level <15 mEq/L, and pH <7.3 with moderate ketonemia constitute the diagnosis.
Patients who present just after receiving insulin or who have impaired gluconeogenesis (alcohol abuse or liver failure) may have lower initial serum glucose levels. Elevated serum levels of HB and AcAc cause acidosis and ketonuria. The nitroprusside reagent normally used to detect urine and serum ketones only detects AcAc; acetone is only weakly reactive and HB not at all. NADH accumulation in mitochondria, as may occur with lactic acidosis or alcohol metabolism, favors the HB side of equilibrium noted earlier (AcAc + NADH ⇌ HB + NAD). The enzymatic test for HB is reliable but not widely available. Paradoxically, as the patient is being treated and clinically improves, measured ketone levels will increase as the body converts the more acidic HB to AcAc. Serum electrolytes should be examined carefully for multiple metabolic abnormalities. Elevated serum ketone levels lead to a wide anion gap metabolic acidosis. Hyperchloremic acidosis also occurs on the basis of ketoanion exchange for chloride in the urine and is especially common in patients who maintain good hydration status and glomerular filtration rate despite ketoacidosis. Metabolic alkalosis also can occur secondary to vomiting, osmotic diuresis, and concomitant diuretic use.
Some patients with DKA may present with normal-appearing [HCO3–] or even an elevated [HCO3–], if coexisting metabolic alkalosis is severe enough to mask the acidosis. In such situations, an elevated anion gap may be the only clue to the presence of an underlying metabolic acidosis otherwise masked by the concomitant volume contraction-related metabolic alkalosis.
According to James G Adam Emergency Medicine (co-author of Rosen) page 1744 :
1.No single standard lab diagnosis for DKA..however any diagnosis for DKA should include
a.Glucose >250mg/dl
b.Elevated beta hydroxybutyrate
c.At least two of the following
-ph < 7.3
-Serum bicarobonate <18 mmol/l (tintenelli 7th bicarbonate<15mmol/l)
-Anion gap> 15 mEq/L (tintenelli 7th anion gap >10)
2.It should be stress that the diagnosis of DKA is mainly based on clinical findi


Ottawa ankle rules:
1.An ankle x-ray is required only if there is any pain in malleolar zone and any of these findings:
a.Bone tenderness along the distal 6 cm of the posterior edge of the tibia or tip of the medial malleolus, OR
b.Bone tenderness along the distal 6 cm of the posterior edge of the fibula or tip of the lateral malleolus, OR
c.An inability to bear weight both immediately and in the emergency department for four steps.
2.A foot x-ray is required if there is any pain in the midfoot zone and any of these findings:
a.Bone tenderness at the base of the fifth metatarsal (for foot injuries), OR
b.Bone tenderness at the navicular bone (for foot injuries), OR
c.An inability to bear weight both immediately and in the emergency department for four steps.
In medicine, the Ottawa ankle rules are a set of guidelines for doctors to aid them in deciding if a patient with foot or ankle pain should be offered X-rays to diagnose a possible bone fracture. Before the introduction of the rules most patients with ankle injuries would have been X-rayed. However only about 15% of X-rays were positive for fracture, other patients had sprains or other injuries. As a result many unnecessary X-rays were taken, which was costly, time consuming and a possible health risk.
Utility of the Ottawa rules:
The rules have been found to have a very low rate of false negatives. Evidence in systematic reviews supports the Ottawa ankle rules as an accurate instrument for excluding fractures of the ankle and mid-foot. The instrument has a sensitivity of almost 100% and a modest specificity, and its use should reduce the number of unnecessary radiographs by 30-40%.
Among the studies in the original review their research reported that the test was 100% sensitive and reduced the number of ankle X-rays by about 35%. A second trial with a larger number of patients confirmed these findings.[4] Subsequently, a multi-centre study was done that explored the feasibility of implementing the rules on a wider scale.Unfortunately, teaching the rules to patients does not appear to help reduce presentation to hospital.
History:
The Ottawa ankle rules were developed by a team of doctors in the Urgent Care department of the Ottawa Hospital in Ottawa, Canada.[3] Since the rules were formulated in Ottawa they were dubbed the Ottawa ankle rules by their creators a few years after their development, a title that has stuck.[4] In this respect, the naming of the rules is similar to that of the Bristol stool scale or the Glasgow Coma Scale (GCS), which also take their names from the cities in which they were formulated.
Conclusion: Evidence supports the Ottawa ankle rules as an accurate instrument for excluding fractures of the ankle and mid-foot. The instrument has a sensitivity of almost 100% and a modest specificity, and its use should reduce the number of unnecessary radiographs by 30-40%. (BMJ 326 : 417 doi: 10.1136/bmj.326.7386.417 (Published 22 February 2003)
Cryoprecipitate = 5ml/kg
Platelet= 10ml/kg
...1 unit=60ml
FFP: 10-20ml/kg
...1 bag=230ml
Packed Cells= 4ml/kg

www.circ.ahajournals.org/cgi/content/full/98/18/1937
The J point in the ECG is the point where the QRS complex joins the ST segment. It represents the approximate end of depolarization and the beginning of repolarization as determined by the surface ECG. There is an overlap of 10 milliseconds. The J point may deviate from the baseline in early repolarization, epicardial or endocardial ischemia or injury, pericarditis, right or left bundle-branch block, right or left ventricular hypertrophy, or digitalis effect. The term J deflection has been used to designate the formation of the wave produced when there is a large, prominent deviation of the J point from the baseline. The J deflection has been called many names, including camel-hump sign, late delta wave, J-point wave, and Osborn wave. 
© Blogger templates Newspaper III by Ourblogtemplates.com 2008
Back to TOP